Arkansas has one of the highest maternal mortality rates in the nation, making it one of the riskiest places to have a baby. Our state also has one of the highest infant mortality rates. This page highlights key statistics and other information about maternal and infant health in Arkansas. It is intended to raise awareness, promote discussion, and inform policymakers and stakeholders as they engage with this issue to make our state a healthier place for mothers and infants.
The Healthy Birthing Journey Podcast is a nine-part series in which we explore the data and issues behind maternal and infant health in Arkansas by speaking with the people working to improve outcomes for moms and babies across our state.
Each episode focuses on one of nine points on the birthing journey, from pre-pregnancy through delivery and into the postpartum period, where ACHI analysts and researchers have identified opportunities for Arkansas to make lasting improvements.
The Healthy Birthing Journey Podcast: Education and Supports
In the third episode of the Healthy Birthing Journey Podcast, we discuss the role of education and support networks for pregnant women in Arkansas and how they contribute to better maternal and infant health outcomes.
The Healthy Birthing Journey Podcast: Prenatal Care
In the second episode of the Healthy Birthing Journey Podcast, we explore the importance of beginning prenatal care early in a pregnancy and speak with healthcare leaders working to remove barriers, increase access, and improve outcomes for Arkansas moms and their babies.
The Healthy Birthing Journey Podcast: Pre-Pregnancy Preparation
Healthy moms begin as healthy women. In the first episode of the Healthy Birthing Journey Podcast, we focus on pre-pregnancy preparation and speak with several healthcare leaders working to improve outcomes for Arkansas moms and their babies.
Our infographic, 9 Points on a Healthy Birthing Journey, depicts what that journey for new mothers should be in order to achieve better maternal and infant health outcomes.
The obstetrics and gynecology (OB-GYN) physician workforce plays a critical role in meeting a wide range of women’s health needs, including maternity care and gynecologic services such as preventive screenings. A lack of available and accessible maternity care is a risk not only at the time of delivery but throughout the birthing journey. Nationwide in 2021-2022, there were 3.8 OB-GYNs for every 10,000 women, according to KFF. Workforce challenges in obstetrics and gynecology can be especially acute in mostly rural states such as Arkansas, which has one of the highest maternal mortality rates in the nation. Recent closures of hospital and obstetric units in Arkansas and around the U.S. also contribute to these challenges.
To better understand the state of OB-GYN care, we have created an interactive dashboard to examine this workforce in Arkansas for the years 2019 through 2022. The dashboard provides visualizations at the state, county, and regional levels and includes information on physician demographics and activity status (full-time, part-time), and payer mix.
Key findings based on data for 2022, the most recent year available, include:
10 counties had no active OB-GYNs.
There were 272 active OB-GYNs in the state, or 3.2 per 10,000 women ages 12-55 residing in Arkansas (based on National Center for Health Statistics population estimates).
About 25% of OB-GYNs were active fewer than 150 days during the year. An “active day” is defined as a day in which the physician provided services to at least two female patients or performed a qualifying procedure.
23% of full-time OB-GYNs were 60 or older, raising concerns about future supply as many approached retirement.
Early-career OB-GYNs (under age 45) were more likely to practice full-time during the year compared to OB-GYNs age 45 and up (88% vs 69%).
The OB-GYN workforce overall was 53% male and 47% female, but among physicians under age 45, 3 out of 4 were women.
While Black and Hispanic Arkansans made up 14.9% and 8.8%, respectively, of the state’s population, they represented only 7% and 2%, respectively, of active OB-GYNs.
The dashboard is intended to inform policymakers, healthcare leaders, and other stakeholders about the supply, characteristics, and distribution of OB-GYNs so they can make evidence-based decisions regarding provider access across Arkansas communities.
Severe Maternal Morbidity in Arkansas
As part of ACHI’s continuing effort to examine each step of the birthing journey in Arkansas, we developed an infographic highlighting the impact of severe maternal morbidity (SMM), defined by the Centers for Disease Control and Prevention as “unexpected outcomes of labor and delivery that result in significant short- or long-term health consequences.” Examples include sepsis, acute renal failure, and acute heart failure.
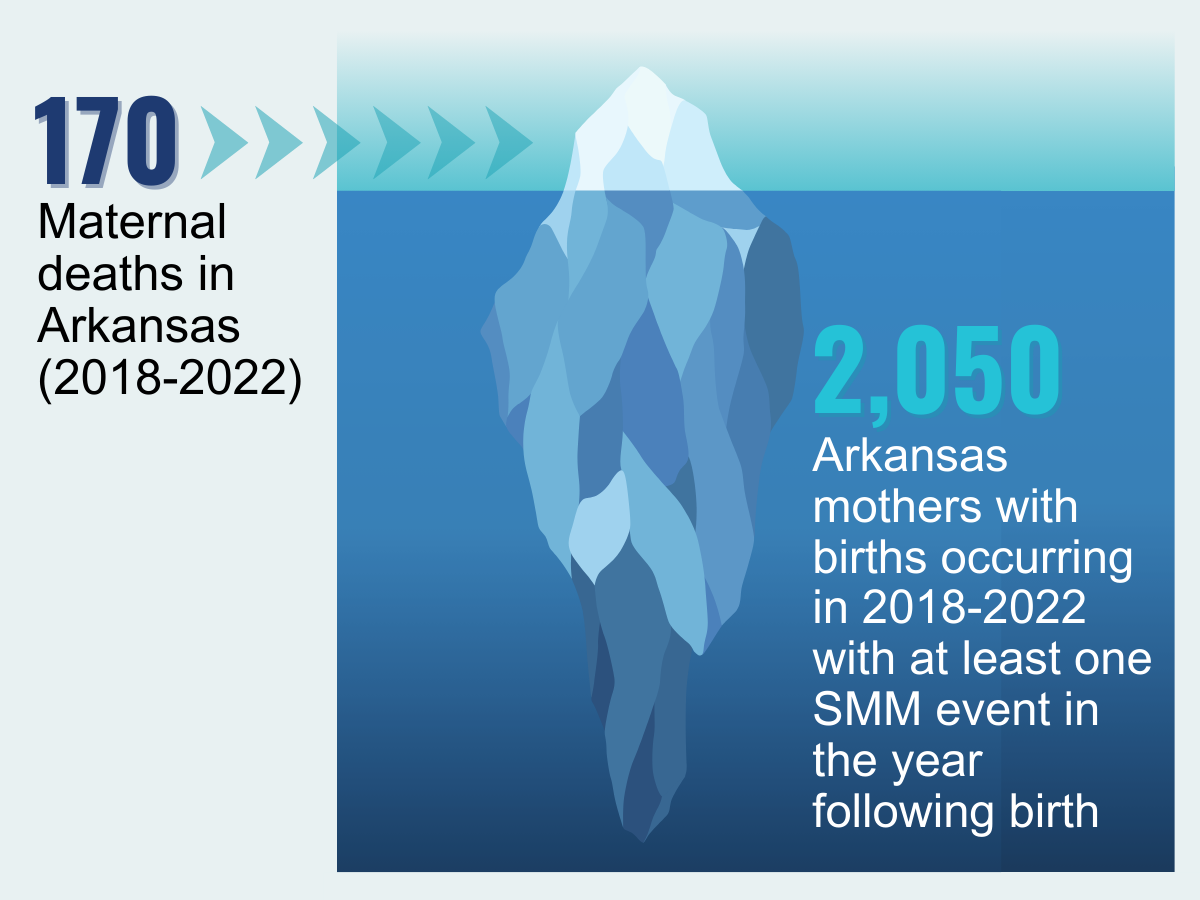
Maternal mortality has been described as the “tip of the iceberg” and severe maternal morbidity as the base. SMM events, also known as maternal near-miss events, occur much more frequently than maternal deaths despite receiving less public attention.
ACHI analyzed hospital discharge data for births that occurred between 2018 and 2022 to determine the impact of SMM among those mothers up to one year postpartum.
Key findings:
While 170 maternal deaths occurred in Arkansas between 2018 and 2022, 2,050 women who gave birth during that period experienced at least one SMM event up to a year after birth.
Between 2018 and 2022, for every 1,000 birth events (i.e., hospitalizations during which at least one delivery occurred) in Arkansas, 13.4 were associated with at least one SMM event.
SMM events most commonly occurred during birth (42.4%), but 35.6% occurred more than six weeks after discharge, 12.2% occurred two to six weeks after discharge, and the remaining 9.7% occurred within a week after discharge.
The five most common types of SMM events were sepsis (3.4 per 1,000 birth events), adult respiratory distress syndrome (2.6 per 1,000 birth events), acute renal failure (2.6 per 1,000 birth events); pulmonary edema/acute heart failure (2 per 1,000 birth events); and hysterectomy (1.8 per 1,000 birth events).
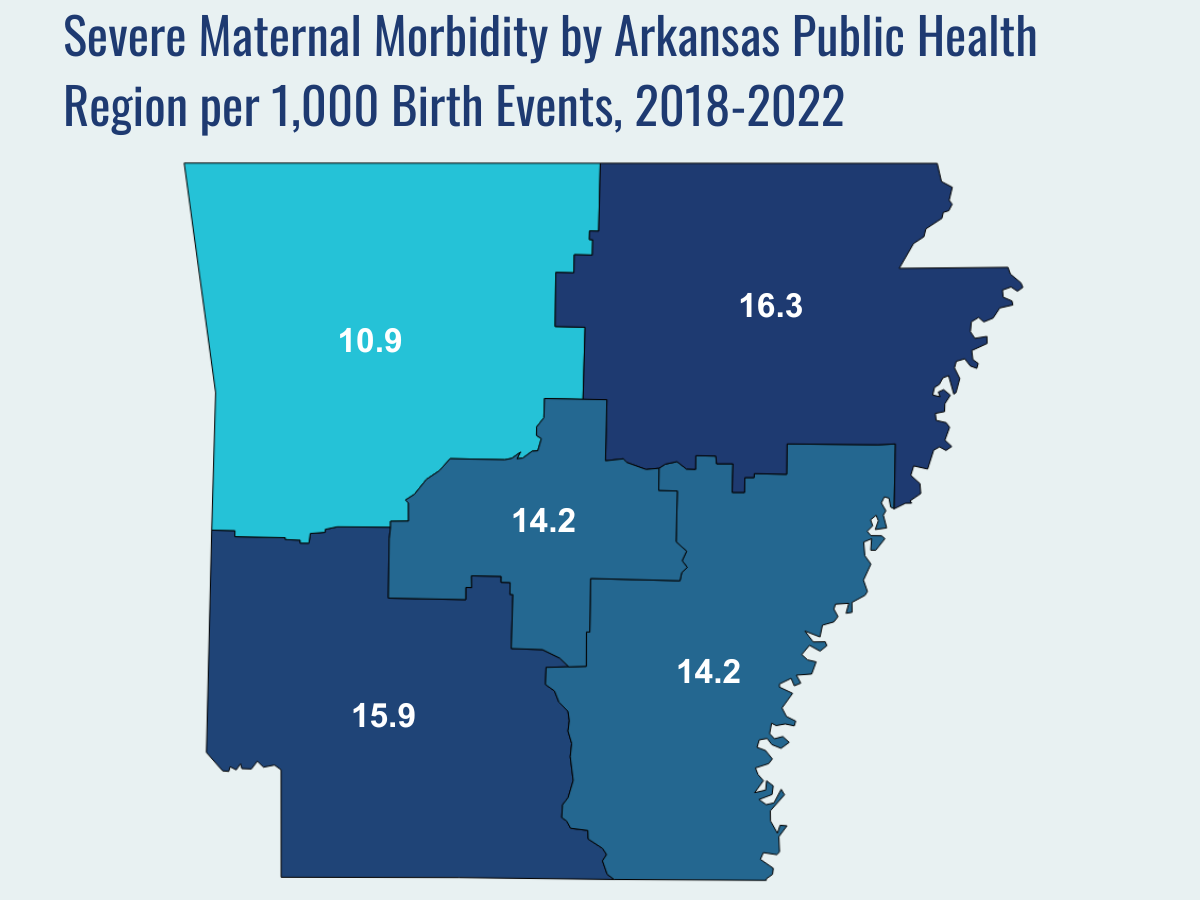
Geographically, SMM events were most common in the Northeast Public Health Region (16.3 per 1,000 birth events), followed by the Southeast Region (15.9 per 1,000 birth events), the Southwest Region and the Central Region (14.2 per 1,000 birth events in both), and the Northwest Region (10.9 per 1,000 birth events).
By age, SMM events were most common among women 40 and older (29.1 per 1,000 birth events), followed by women ages 35-39 (20.7 per 1,000 birth events), women ages 30-34 (13.6 per 1,000 birth events), women under 20 (12.6 per 1,000), women ages 25-29 (11.8
By race and ethnicity, SMM events were most common among Black women (20.7 per 1,000 birth events), followed by women whose race was identified as Pacific Islander/American Samoa (19 per 1,000 birth events), women of unknown race or ethnicity (14.7 per 1,000 birth events), American Indian/Alaskan Native women (12.6 per 1,000 birth events), White women (12.2 per 1,000 birth events), Asian women (10 per 1,000 birth events), and Hispanic women (9.5 per 1,000 birth events).
Dashboard: Arkansas Obstetrics and Gynecology (OB-GYN) Physician Workforce
Severe Maternal Morbidity in Arkansas
100 ARKANSAS MOMS
The health of a mother can play a significant role throughout the birthing journey. As part of ACHI’s 100 Arkansans initiativeto illustrate demographic and health statistics, we examined important risk factors among Arkansas moms from pre-pregnancy through postpartum, including recent healthcare visits, access to insurance coverage, body mass index, tobacco use, vaccinations, and other factors.
Data for the infographic are from the Centers for Disease Control and Prevention’sPregnancy Risk Assessment Monitoring System. New moms are defined as women who gave birth two to four months prior to survey administration. Arkansas data for 2017 were not available.
More than half of rural hospitals in the U.S. no longer offer labor and delivery services, according to a report by the Center for Healthcare Quality and Payment Reform. At many hospitals that continue to offer labor and delivery services, those services are at risk due to challenges with the healthcare workforce and hospital finances that increasingly make it difficult to subsidize these departments, which are required to remain fully staffed 24 hours a day, seven days a week.
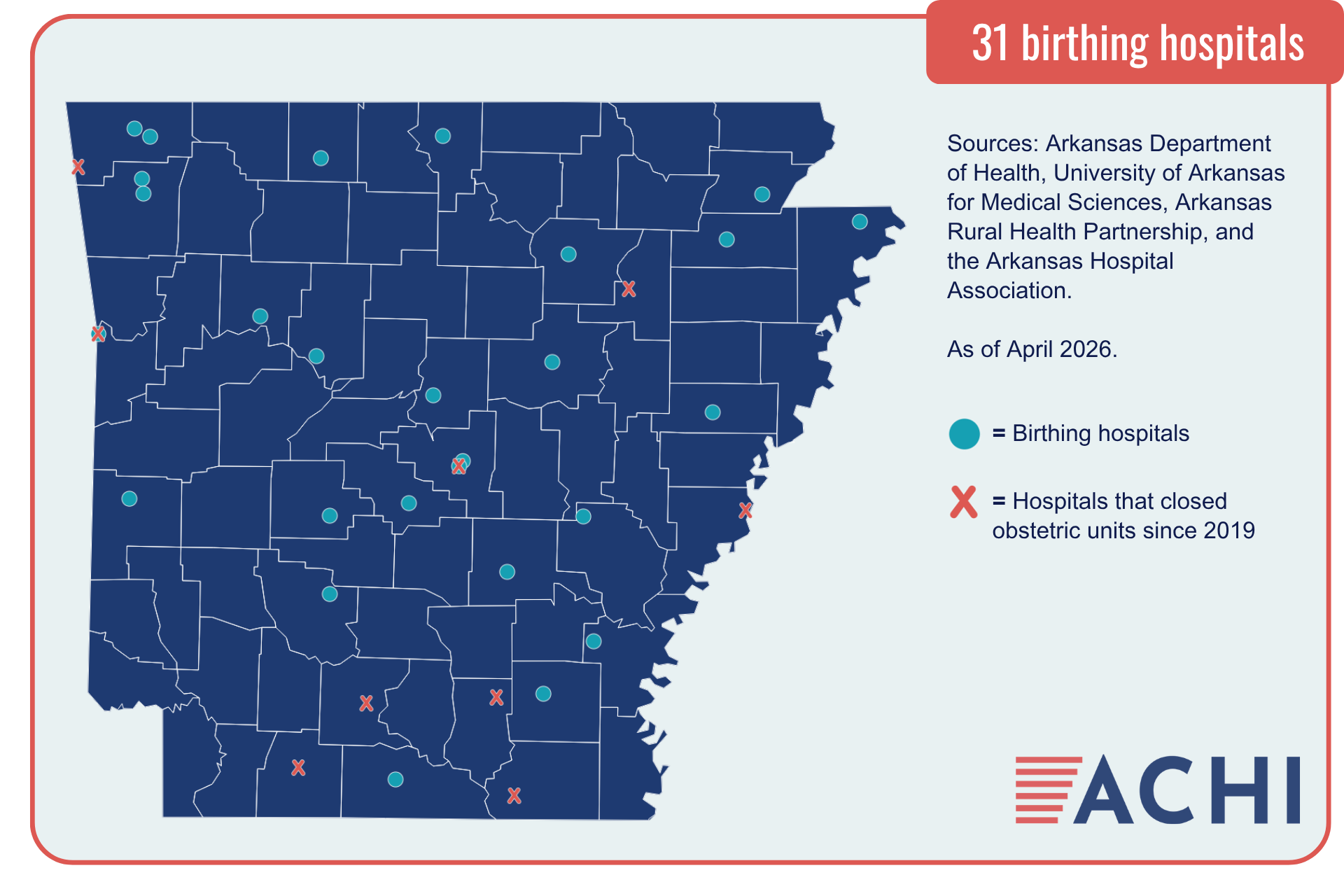
ACHI has identified 31 Arkansas hospitals that provide labor and delivery services. Nine hospitals in the state have closed their obstetric units since 2019. Among the state’s rural hospitals, 60% do not offer these services, which means expecting mothers must travel farther to deliver a child and receive appropriate prenatal and postpartum care, key points on a healthy birthing journey.
As of April 2026, Arkansas hospitals that provide labor and delivery services include:
Arkadelphia: Baptist Health Medical Center
Batesville: White River Medical Center
Benton: Saline Memorial Hospital
Bentonville: Northwest Medical Center
Blytheville: Great River Medical Center
Clarksville: Johnson Regional Medical Center
Conway: Baptist Health Medical Center
Conway: Conway Regional Health System
Dumas: Delta Memorial Hospital
El Dorado: South Arkansas Regional Hospital
Fayetteville: Washington Regional Medical Center
Forrest City: Forrest City Medical Center
Fort Smith: Mercy Hospital Fort Smith
Harrison: North Arkansas Regional Medical Center
Hot Springs: CHI St. Vincent Hot Springs
Hot Springs: National Park Medical Center
Johnson: Willow Creek Women’s Hospital
Jonesboro: NEA Baptist Memorial Hospital
Jonesboro: St. Bernards Medical Center
Little Rock: Baptist Health Medical Center
Little Rock: University of Arkansas for Medical Sciences
Mena: Mena Regional Health System
Monticello: Baptist Health Medical Center – Drew County
Mountain Home: Baxter Regional Medical Center
North Little Rock: Baptist Health Medical Center
Paragould: Arkansas Methodist Medical Center
Pine Bluff: Jefferson Regional Medical Center
Rogers: Mercy Hospital Northwest Arkansas
Russellville: Saint Mary’s Regional Health System
Searcy: Unity Health White County Medical Center
Stuttgart: Baptist Health Medical Center
Travel Time to Delivery Facilities for Arkansas Mothers
Closures of labor and delivery services at Arkansas hospitals in recent years have led to longer travel times for many Arkansas mothers. Increased travel times to delivery facilities have been associated with higher risks of adverse maternal and neonatal outcomes. ACHI reviewed data on birth events occurring from 2016 to 2022 to estimate the travel times to delivery facilities for Arkansas mothers.
Our findings are presented in this infographic, which focuses on what we have identified as the fourth step of a healthy birthing journey: accessing safe delivery options.
The statewide median minutes traveled to delivery facilities in 2022 was 16 minutes, but a look at mothers’ median travel times by county of residence found that travel times ranged from as short as 2 minutes to as long as 73 minutes.
In some counties, increases in median travel times for residents followed the closure of local labor and delivery units. The infographic highlights Columbia and Phillips counties as examples of this phenomenon.
The percentages of mothers facing extended travel times for delivery services have increased, with 28% of mothers traveling 30 minutes or more in 2022, up from 26% in 2016, and 8% of mothers traveling 60 minutes or more in 2022, up from 7% in 2016.
The data sources for these analyses were Arkansas Department of Health birth records (for in-state births) and the Arkansas Healthcare Transparency Initiative’s All-Payer Claims Database (for out-of-state births). Travel times were estimated using mothers’ home ZIP codes and the addresses of delivery facilities.
Following the April closure of a local labor and delivery unit in Fort Smith, ACHI President and CEO Craig Wilson spoke with the Times Record about the increasing financial pressures faced by Arkansas hospitals and the impact such closures have on access to maternal health resources.
ACHI Health Policy Director Jennifer Wessel spoke with 40/29 News in April about the impact labor and delivery unit closures can have on rural Arkansas communities and efforts underway at the state level to support maternal health.
ACHI Health Policy Director Jennifer Wessel spoke with the Oxford American about evolving maternal health challenges facing rural Arkansas communities.
Related Blog Posts
10 Years of Data Collection, Analysis, and Research Through the Arkansas Healthcare Transparency Initiative
Research Notes: Impact of Medicaid Nutrition Support on Healthcare Utilization, Costs
State, Federal Health Policy Changes Set To Take Effect in 2026
Tracking Respiratory Illness Trends, Vaccination Rates as Winter Approaches
Assessing Rural Primary Care Challenges, Solutions
How Some Rural Communities Have Maintained Access to Maternity Care
Related News Releases
The current query has no posts. Please make sure you have published items matching your query.