



Background
A CHW is generally a community member who is involved in improving the overall health of the community, either in a position of employment or on a voluntary basis. CHWs are integrated within the communities they serve and typically help to address both the clinical and non-clinical needs of patients. CHWs act as a link between healthcare providers and community members and may provide services such as coordinating care, offering health education, and acting as patient navigators within the healthcare system. The U.S. Bureau of Labor Statistics estimates that there were 65,100 CHWs employed in the U.S. as of 2024 and projects employment of CHWs to increase by 11% from 2024 to 2034, a much faster growth rate than the average across all occupations.1
Evidence on the Effectiveness of Community Health Workers
Numerous studies have explored the effectiveness of CHWs in various settings. Research indicates that CHWs can improve health outcomes and access to care, particularly among underserved and vulnerable populations. A summary of systematic reviews found that CHW-led interventions appear more effective than alternative approaches and can be cost-effective for certain health conditions, especially when focused on underserved communities.2
There is also evidence that CHWs may reduce healthcare costs. One example is the Kentucky Homeplace program, which has trained CHWs since 1994 and serves rural counties in the Appalachian region of the state. Clients served by the program are typically at 100%-133% of the federal poverty level and receive a variety of services, such as chronic disease management, health coaching, help accessing medications and medical supplies, and referrals to health and social services. The program reports an estimated return on investment of $11.31 saved for every dollar invested.3
CHWs also help to reduce avoidable hospitalizations by addressing patient health issues before they become serious. A randomized controlled trial of nurse care manager and CHW interventions found that patients who received both interventions had the greatest improvements in blood sugar control and other diabetes-related risk factors compared with patients who received only one intervention or usual care.4 CHWs may also increase the efficiency of healthcare systems by providing services such as routine health screenings, allowing clinical providers to target patients with more complex care needs.
There is also evidence that CHWs can help to improve the cultural competency and responsiveness of healthcare systems.5 CHWs often come from the same communities as the patients they serve and can provide a more personalized and culturally appropriate approach to care. CHW and patient navigation programs have been used in rural community settings. For example, in a South Dakota-based patient navigation program intended to reduce cancer disparities among American Indians, patients who received navigation services during cancer treatment had an average of three fewer days of treatment interruptions than patients who did not receive navigation services.6
Training and Certification of Community Health Workers
There is no standardized national curriculum or set of core training methods for CHWs, although the National Council on CHW Core Consensus Standards, or National C3 Council,7 a working group of experienced professionals in the field, has recommended a set of roles and core competencies for community health workers. In lieu of national standardization, many states have developed their own training and licensure requirements.
In Arkansas, CHW training has historically been supported by the Arkansas Community Health Worker Association (ARCHWA), which was founded in 2013. Act 435 of 2025 named the association, in conjunction with the Arkansas Division of Higher Education, as the entity responsible for creating and maintaining a public registry of approved CHW training programs.8 Act 435 also established a statewide CHW certification program overseen by the Arkansas Department of Health (ADH).8
Proposed ADH rules would establish a state certification program for CHWs in Arkansas. Act 435 ties certification under that program to eligibility for Medicaid or private insurance reimbursement for CHW services.9 CHW certification would be valid for two years. Applicants would have to be at least 18, submit an application, provide certain documentation, meet one of the eligibility pathways listed below, and pay a $50 initial certification fee. Renewal would require 20 hours of professional development or training every two years and a $50 renewal fee. The proposed rules also include provisions establishing automatic certification for certain uniformed service members, veterans, and their spouses; reciprocal certification for substantially equivalent out-of-state certification or licensure; disciplinary actions; conditions for inactive status, reactivation, and expiration; and ADH responsibilities.
The proposed rules include several pathways to certification, recognizing both formal training and prior work experience. This structure would tie certification to common training and competency expectations while allowing individuals with different backgrounds to qualify.
TABLE 1: PROPOSED ARKANSAS CHW CERTIFICATION PATHWAYS
| Pathway | Eligibility Requirements |
|---|---|
| Existing ARCHWA certification. | Applicant is already certified as a CHW by ARCHWA. |
| Completion of training program plus two years of experience. | Applicant has worked as a CHW for two years, including one year in Arkansas, and completed a 120-hour CHW training program from an approved school or training program. The 120 hours must include 80 hours of didactic training and 40 hours of guided field practice. Most closely aligns with ARCHWA’s traditional track. |
| Experience plus supplemental training, mentorship, and supervision. | Applicant has worked as a CHW for one year in Arkansas and completed 80 hours of supplemental training supporting core competency and professional development. The applicant also must have a CHW mentor and a supervisor who has completed CHW supervisor training, with regular documented communication. Most closely aligns with ARCHWA’s apprenticeship track. |
| Four years of experience demonstrating core competencies. | Applicant has four years of CHW experience showing proficiency in core competencies, including two years of experience in Arkansas. Most closely aligns with ARCHWA’s experiential track. |
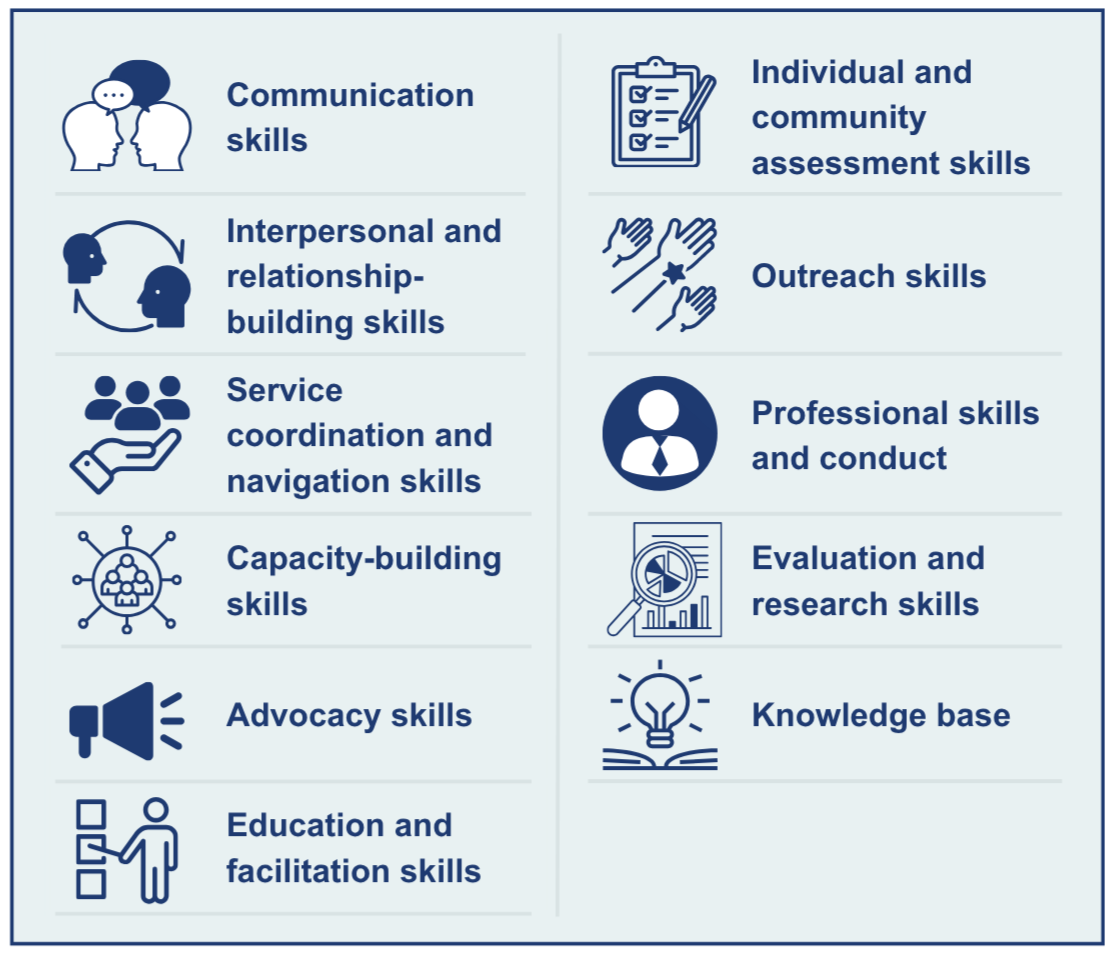
Arkansas-certified CHWs are expected to demonstrate core competencies (see Figure 1) that align with national standards for CHW roles and responsibilities, including communication, care coordination, health education, system navigation, advocacy, capacity building, individual and community assessment, outreach, and participation in evaluation and research activities.10 These competencies provide the foundation for CHW training and help define the services CHWs may provide in healthcare and community settings.
FIGURE 1: CORE COMPETENCIES OF ARKANSAS-CERTIFIED COMMUNITY HEALTH WORKERS
MEDICAID
State Medicaid programs take varying approaches to reimbursing CHW services.
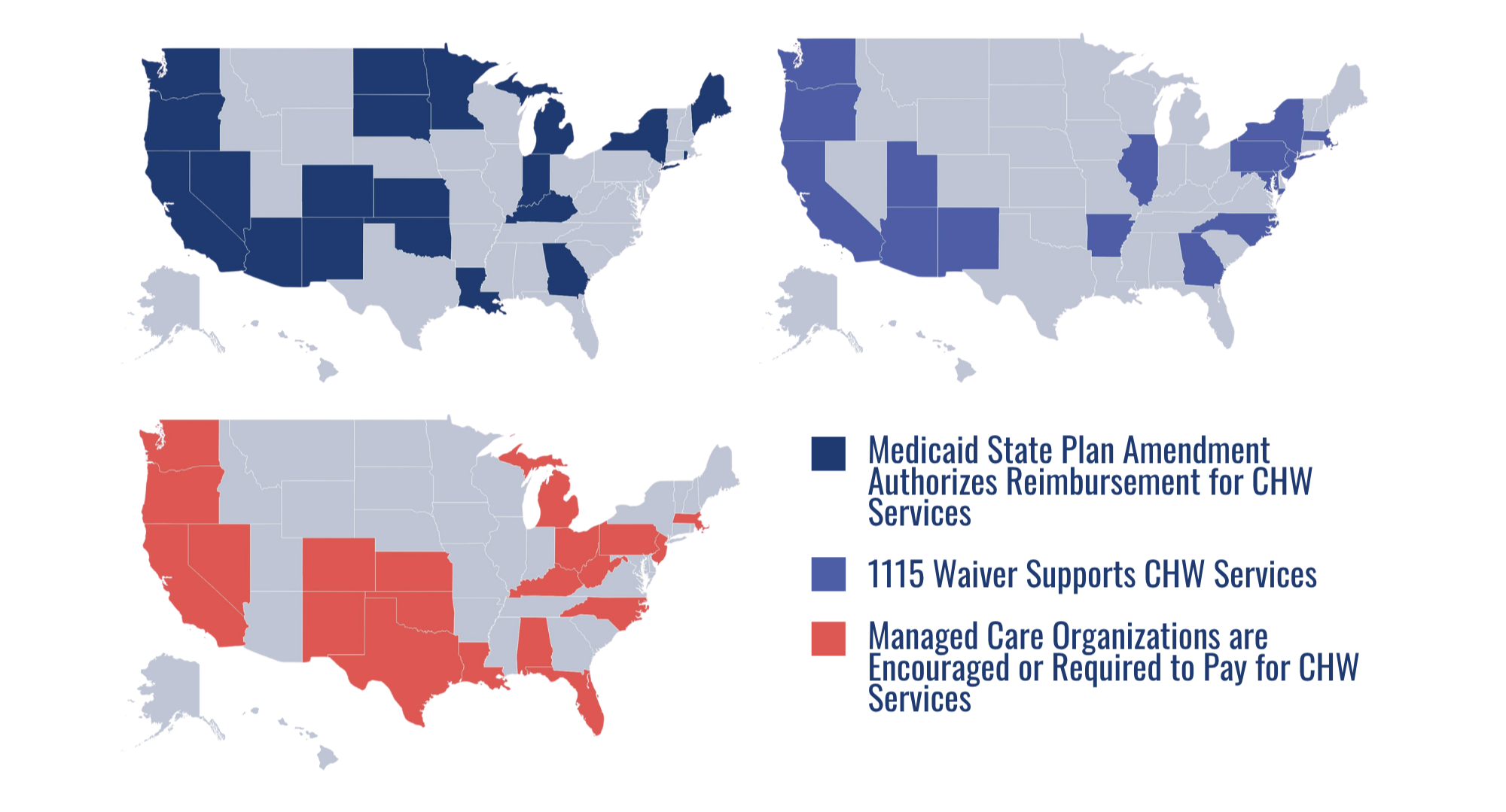
States may pursue coverage of CHW services by amending their state Medicaid plans; by exercising Section 1115 demonstration waiver authority, which allows states to test new and innovative programs; or by requiring or encouraging managed care organizations to render CHW services or include CHWs in patient care teams.11 Arkansas will join 20 other states that have received Centers for Medicare and Medicaid Services (CMS) approval for Medicaid state plan amendments authorizing reimbursement for CHW services.12
FIGURE 2: STATE APPROACHES TO FUNDING MECHANISMS FOR COMMUNITY HEALTH WORKER SERVICES13
In Arkansas, Medicaid reimbursement for CHW services is tied to broader statewide efforts. Act 140 of 2025, the Healthy Moms, Healthy Babies Act, requires Medicaid reimbursement for CHW home visitation related to prenatal and postpartum care. Act 435 creates a broader reimbursement pathway by requiring compensation for certified CHWs through Medicaid or private health insurance.
While these laws authorize reimbursement, Medicaid implementation will require additional state and federal steps. These steps include finalizing ADH certification rules and Medicaid coverage requirements, obtaining any needed federal approval, and completing required public and legislative review processes.
Other implementation issues include establishing which CHW services Medicaid will cover; which providers or entities may bill for those services; how supervision or care team requirements will be structured; whether beneficiary exclusions or benefit limits will apply; what documentation will be required; and how payment rates will be set. Federal Medicaid rules set standards for state payment methodologies to ensure they are reasonable, support quality care, and allow Medicaid beneficiaries access to covered services. National guidance notes that Medicaid fee-for-service rates for CHW-related services vary widely across states, ranging from just over $18 to $50 per 30-minute unit as of January 2025.14
OTHER PAYERS
Medicare has expanded payment pathways for services that may involve CHWs, but payment generally flows through an eligible billing practitioner or provider organization rather than directly to the CHW. The 2024 Medicare Physician Fee Schedule final rule established payment for community health integration (CHI) services.15 These services may be provided by certified or trained auxiliary personnel, including CHWs, under the direction of a billing practitioner. CHI services are intended to address health-related social needs that affect a patient’s diagnosis or treatment, including care coordination, health education, system navigation, and connections to community-based services.
Subsequent Medicare policy changes have continued to support team-based care models that may include CHWs or CHW-adjacent roles. The 2025 Medicare Physician Fee Schedule final rule created new coding and payment for advanced primary care management services and finalized opioid treatment program add-on codes — billing codes that allow additional payment for specified services — for coordinated care and referral services, patient navigation services, and peer recovery support services.16 The 2026 Medicare Physician Fee Schedule final rule replaced the term “social determinants of health” with “upstream drivers” in CHI-related policies, a change that is intended to better describe the range of social, behavioral, environmental, and medical factors that can affect health outcomes.17 Although these changes still do not allow CHWs to bill Medicare directly, they may support CHW-related functions in primary care, behavioral health, and substance use treatment settings.
Private insurance coverage for CHW services has historically varied by payer and plan. In Arkansas, Act 435 requires private insurers to compensate certified CHWs for providing services.18 Operational details for private insurers will likely depend on plan filings, insurer policies, and any additional state guidance.
Investment in Community Health Worker Services
Investment in CHW services increasingly comes from a mix of federal and state sources. In Arkansas, recent activity has focused not only on reimbursement but also on workforce development and integration of CHWs into maternal health and public health settings. The University of Arkansas for Medical Science’s Institute for Community Health Innovation has supported CHW workforce development through training programs for new and experienced CHWs across Arkansas.19 In 2025, the institute received $375,000 from the Arkansas Office of Skills Development to train 75 CHWs over 18 months, with a focus on rural counties. CHWs are supporting the University of Arkansas for Medical Sciences’ Proactive Postpartum Call Center, which connects postpartum patients with follow-up support, referrals, and health-related social needs.20 Arkansas’s Transforming Maternal Health grant, which supports implementation of a federal maternal health model focused on improving pregnancy, birth, and postpartum care, and the state’s HEART Moms (Helping Expand Access to Rural maternal health care Transformation for Moms) initiative, a rural maternal health effort focused on improving access to care in South Arkansas, include efforts to expand or strengthen CHW roles in perinatal and maternal health care.21,22 The Arkansas Rural Health Partnership is also listed by ARCHWA as an approved CHW core competency training provider, reflecting the broader role of rural health partners in building the CHW workforce.23 The long-term sustainability of CHW services will likely depend on whether these roles can be supported through stable reimbursement and workforce funding rather than grant funding alone.
